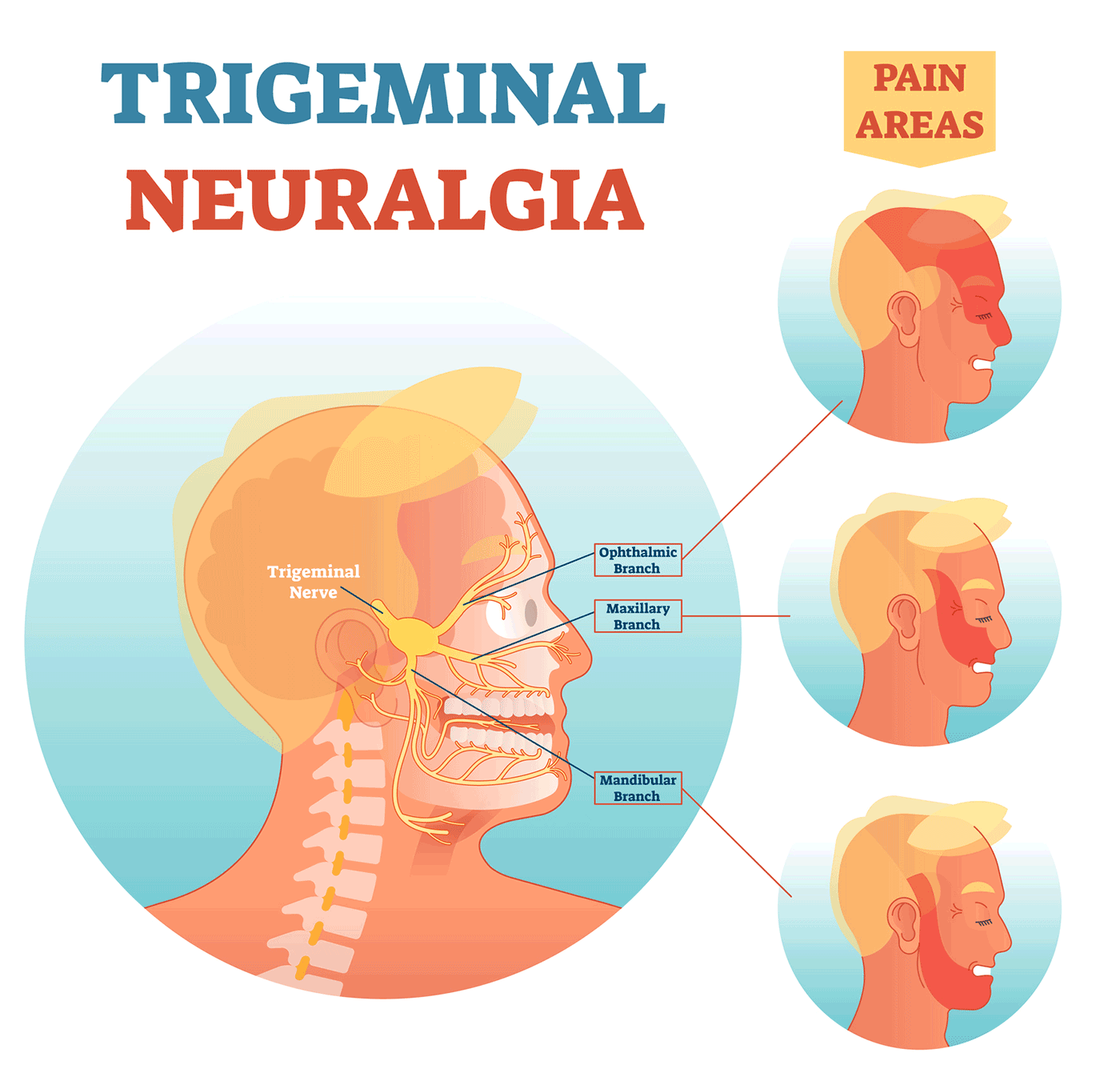
Typical Trigeminal Neuralgia is characterized by lancinating electric-shock like pain down one side of the face, in one/more divisions of the trigeminal nerve. Pain in the maxillary and mandibular divisions is often confused with pain of dental origin. Though it is a benign disorder, the pain can be severe enough to drive one to suicide and therefore, Trigeminal Neuralgia is called the “suicide disease”.
Pain in the maxillary and mandibular divisions is often confused with pain of dental origin. In the process, patients often get multiple dental treatments done without any relief in pain before the diagnosis is finally made.
Radiology for Trigeminal Neuralgia serves two purposes. The first is to rule out a secondary cause of trigeminal neuralgia, such as tumors in the petroclival region. The second purpose is recognition of a vascular loop at the root entry zone of the fifth/trigeminal nerve where the nerve enters the brainstem.
The mainstay of medical treatment of Trigeminal Neuralgia is Carbamazepine/Oxcarbamazepine. As a matter of fact, typical trigeminal neuralgia will always initially respond to Carbamazepine/Oxcarbamazepine. Response to Carbamazepine/Oxcarbamazepine is considered a diagnostic feature of typical trigeminal neuralgia. Once Carbamazepine fails, no other medical treatment is really effective though partial success can be achieved with Pregabalin.
It is important not to delay referral for other modes of treatment once Carbamazepine/Oxcarbamazepine fails because severe pain can push patients to the brink of suicidal attempts.
Therefore, once Carbamazepine/Oxcarbamazepine fails, an interventional/surgical cure becomes paramount. The first step in this direction would be to order a MRI tailored to recognize a blood vessel loop at the root entry zone of the fifth/trigeminal nerve where the nerve enters the brainstem. The MRI is best ordered by a Functional Neurosurgeon experienced in Microvascular Decompression surgery for Trigeminal Neuralgia. The most common vessels implicated in Neuro-Vascular compression of the fifth nerve leading to Trigeminal Neuralgia are the superior cerebellar artery and the anterior inferior cerebellar artery.
If a vascular loop is identified on the MRI at the root entry zone of the involved fifth/trigeminal nerve, we offer Microvascular Decompression Surgery as the first treatment of choice to patients, more so if they are young.
What Microvascular Decompression surgery involves is getting to the root-entry zone of the fifth nerve deep inside the brain and separating the compressing vessels from the fifth nerve by interposing either Teflon felt or Goretex vascular graft. This operation is done under an operating microscope and a Neuro-Endoscope is often used alongside to provide vision around corners. This is a technically demanding surgery in a narrow corridor which contains the cerebellum, the brainstem, the superior petrosal vein, the Facial nerve and the Hearing nerves besides the 5th nerve and the offending vessels in contact with the nerve and therefore is best left to a surgeon experienced at such surgery. What is important to understand is that though the MRI may show only one source of neurovascular compression, intraoperatively more sources may be identified, including compressing veins, all of which need to be separated from the nerve.
However, the excellent long-term complete pain relief rates of 80-90% make Microvascular Decompression the most attractive option. The absence of dreaded complications such as anaesthesia dolorosa and corneal anaesthesia/keratitis makes it even more attractive.
I use Goretex cylindrical vascular grafts with an unique spring action to separate the compressing blood vessels from the 5th/trigeminal nerve.
It must be reiterated that Microvascular Decompression Surgery is the gold standard of treatment for Trigeminal Neuralgia. However, the long-term success and risks of complications are highly dependent on the finesse of the operating surgeon.
If the MRI is negative or the patient does not want surgery or is ineligible for surgery for medical reasons, we offer Percutaneous Balloon Microcompression of the fifth nerve at the Meckel’s cave as the treatment of choice.
The most important way Percutaneous Balloon Microcompression differs from the other two more commonly used percutaneous methods of treatment, that is, glycerol rhizotomy and radiofrequency rhizotomy is that balloon microcompression is a non-destructive treatment. The percutaneous methods of treatment are performed via a needle inserted by the side of the mouth under x-ray guidance all the way to the Meckel’s cave which is a small cave at the base of the skull where the 5th /trigeminal nerve branches into 3 divisions to supply one side of the face. The more commonly used percutaneous methods are glycerol rhizotomy whereby glycerol is injected through the needle to chemically damage the nerve and radiofrequency rhizotomy whereby a radiofrequency electrode is used through the needle to electrically damage the nerve. Balloon microcompression is a non-destructive treatment whereby a small balloon is inserted through the needle and inflated for a few minutes to compress the nerve before being deflated and removed.
Being a non-destructive treatment, balloon microcompression does not lead to the deadly complications of glycerol and radiofrquency, Anaesthesia Dolorosa and Corneal anaesthesia/keratitis.
Anaesthesia Dolorosa is a severe de-afferentiation burning pain caused by nerve destruction, as is done with glycerol/radiofrequency. Anaesthesia Dolorosa is probably the most severe pain known to mankind and is also the most difficult to treat. Though the chances of occurrence of Anaesthesia Dolorosa with glycerol/radiofrequency is only around 1-2%, it is enough to re-consider the use of such destructive procedures.
Corneal anaesthesia leading to keratitis and corneal ulcers is a more frequent complication of destructive procedures such as glycerol/radiofrequency while the incidence is almost zero with balloon microcompression.
The largest experience with Balloon Microcompression reveals 81% of patients were found to have complete pain relief at 5 years. This almost rivals the results achieved with Microvascular Decompression. At 10 years, however, 68% of patients were found to have complete pain relief, which is definitely lower than the results achieved with Microvascular Decompression. It is also to be noted here that long-term results of glycerol/radiofrequency are much worse, with most patients requiring repeated injections at regular intervals with decreasing efficacy.
Percutaneous balloon microcompression is done under general anaesthesia because of the significant risk of bradycardia during balloon inflation. Overall, general anaesthesia is also much more comfortable for the patient which in turn makes balloon microcompression all the more attractive since both glycerol and radiofrequency are done with the patient awake and can cause severe discomforting pain to the patient.
Percutaneous balloon microcompression is a more complicated procedure than glycerol/radiofrequency and therefore is more technically demanding with very few doctors in the world performing this intervention.
Gamma Knife Radiosurgery is the other option but we prefer to keep it in reserve as the last resort.
To summarize, a rational, non-destructive, long-term management algorithm for Trigeminal Neuralgia would be a CT/MRI scan followed by Carbamazepine trial. Once Carbamazepine fails, Pregabalin can be tried in combination. If that fails also, the patient requires referral to a Trigeminal Neuralgia specialist. The first step hereafter would be a high-quality tailored MRI to recognize a vascular loop on the offending nerve. If a loop is identified and the patient is relatively young with no gross medical illnesses, Endoscope-assisted Microvascular Decompression of all the offending vessels would offer the best long-term results, but only in the hands of an experienced Functional Neurosurgeon. If no loop is identified, or the patient is elderly or has gross medical illnesses precluding surgery, or does not want surgery, Percutaneous Balloon Microcompression is the preferred option in terms of long-term results and complications rather than destructive procedures such as Glycerol/Radiofrequency Rhizotomy. We keep Gamma Knife Radiosurgery in reserve as the final resort. With such an approach, this “suicide disease” can definitely be alleviated.